

Why hair thins at crown: causes and solutions
Why hair thins at crown: causes and solutions

Androgenetic alopecia is the primary cause of why hair thins at crown, affecting over 50% of men past age 50 and rising to as many as 85% by age 70 in the UK. This hereditary condition causes dihydrotestosterone (DHT) to shrink hair follicles progressively, producing finer, shorter strands until growth stops altogether. The medical term “androgenetic alopecia” is the standard clinical label for what most people call male or female pattern baldness. Understanding the biology behind crown region hair thinning is the first step towards choosing the right response, whether that is medical treatment, lifestyle change, or surgical restoration.
Why does hair thin at the crown? The biology explained
Over 95% of hair loss cases are caused by androgenetic alopecia, driven by genetic sensitivity to DHT. That single statistic explains why crown thinning is so common and why it runs in families.
DHT is a hormone derived from testosterone. In people with genetically sensitive follicles, DHT binds to receptors in the scalp and triggers a process called follicle miniaturisation. The Wnt/β-catenin signalling pathway also plays a role in this process, disrupting the normal signals that keep follicles healthy and active.

Miniaturisation works in stages. Terminal hairs, the thick, pigmented strands you can see clearly, gradually shrink into vellus-like hairs, which are fine, colourless, and barely visible. The anagen (growth) phase shortens with each cycle, while the telogen (resting) phase lengthens. Over time, follicles produce hairs so thin they offer no visible coverage.
The crown is particularly vulnerable because follicles in the vertex region carry a higher density of DHT receptors than follicles at the sides and back of the scalp. This is why the back and sides remain fuller for longer, even in advanced cases. That biological difference is also the reason donor hair from the back of the scalp is used in hair transplant surgery.
Pro Tip: If you notice your hair looking thinner at the top but full at the sides, that asymmetry is a classic early sign of androgenetic alopecia rather than general shedding.
How do male and female crown thinning patterns differ?
Crown thinning patterns differ significantly by sex, and recognising those differences matters for accurate diagnosis and treatment planning.
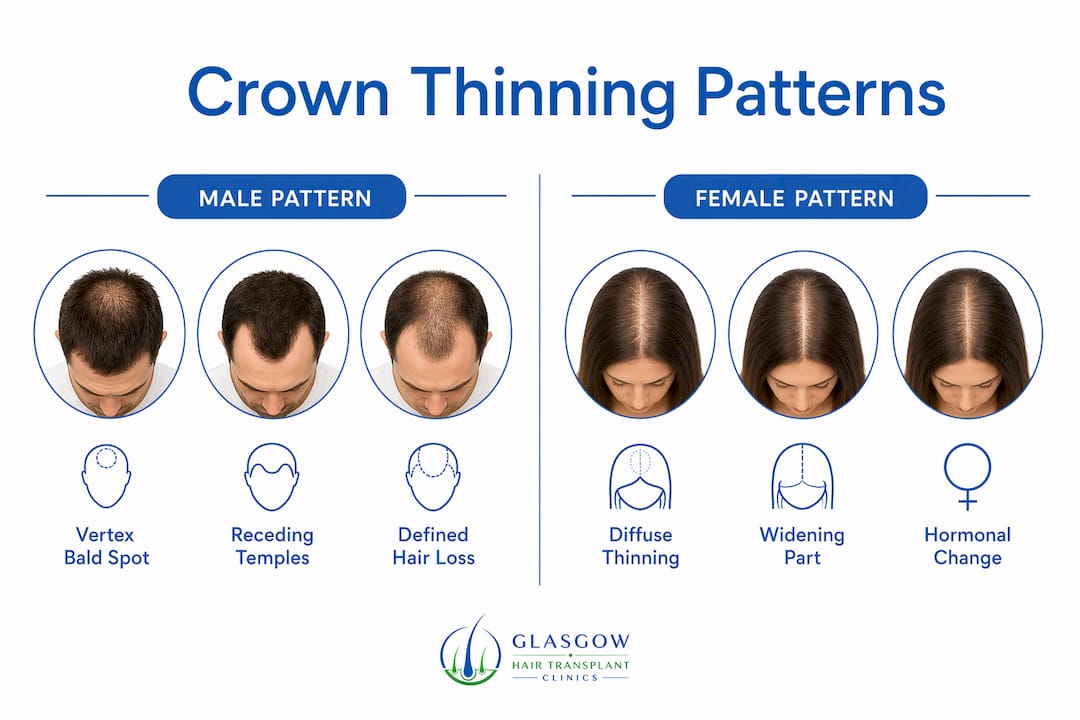
Men typically develop a defined bald spot at the vertex, often alongside a receding hairline at the temples. These two areas can eventually merge, producing the classic horseshoe pattern. Women, by contrast, experience diffuse thinning across the top of the scalp with a widening parting line. The frontal hairline in women is usually preserved, which is why female pattern hair loss is often less immediately obvious to others but no less distressing.
| Feature | Male pattern | Female pattern |
|---|---|---|
| Thinning location | Vertex bald spot, receding temples | Diffuse thinning across the crown |
| Frontal hairline | Often recedes | Usually preserved |
| Progression | Defined, staged (Hamilton-Norwood scale) | Gradual, diffuse (Ludwig scale) |
| Visibility | Bald patch becomes obvious | Widening parting, reduced density |
| Hormonal trigger | DHT sensitivity | DHT plus oestrogen decline |
Women experiencing diffuse crown thinning should also consider hormonal changes, particularly around menopause, when oestrogen levels fall and DHT influence increases. A step-by-step guide for women dealing with this pattern can help clarify which approaches are most appropriate.
Pro Tip: Women who notice a widening parting rather than a receding hairline should request a female-specific assessment. The Ludwig scale, not the Hamilton-Norwood scale, is the correct diagnostic tool for female pattern loss.
What other factors contribute to thinning hair at the top?
Androgenetic alopecia is the dominant cause, but several other factors accelerate or mimic crown hair thinning.
- Telogen effluvium. Acute shedding triggered by illness, rapid weight loss, surgery, childbirth, or emotional stress typically begins 2–3 months after the triggering event and often resolves within 6–9 months once the cause is addressed. When telogen effluvium occurs alongside androgenetic alopecia, the combined effect on the crown can appear severe.
- Medical conditions. Thyroid disease, lupus, and iron deficiency can all manifest as hair thinning. Fatigue, skin changes, or hormonal irregularities alongside hair loss are signals that a GP referral is warranted before starting any hair loss treatment.
- Traction alopecia. Tight hairstyles such as high buns, cornrows, and extensions place repeated mechanical stress on follicles. Over time, this causes permanent follicle damage, particularly along the hairline and crown. The causes and signs of traction alopecia are worth understanding if you regularly wear your hair pulled back tightly.
- Nutritional deficiencies. Low levels of ferritin, vitamin D, and zinc are associated with increased hair shedding. These deficiencies are correctable, which makes them worth testing for before assuming the cause is purely genetic.
- Scalp health and environment. Chronic UV exposure, harsh chemical treatments, and scalp inflammation can weaken follicles over time. A compromised scalp environment accelerates the miniaturisation process in genetically predisposed individuals.
Distinguishing pattern hair loss from systemic illness is critical. Treating androgenetic alopecia when the real cause is thyroid disease, for example, produces no benefit and delays the correct intervention.
How can you detect early signs of crown thinning?
Follicle miniaturisation begins in the late teens or early twenties and progresses gradually. Visible thinning only appears after significant follicle damage has already occurred. That delay is why early detection matters so much.
The crown sits outside the natural line of sight. Most people first notice crown thinning when someone else points it out, or when they catch an indirect reflection. Patients often attribute early changes to styling choices rather than follicle loss.
These steps help you assess your crown objectively:
- Take monthly photographs. Use two mirrors or a smartphone camera held overhead in consistent lighting. Compare images month to month rather than day to day, since daily variation is normal.
- Check hair diameter. Hair diameter reduction is a key early indicator of miniaturisation. If individual strands feel finer than they used to, that change is clinically significant even before visible thinning appears.
- Monitor your parting. A widening parting or increased scalp visibility under direct light signals reduced density.
- Book a professional assessment. A trichologist or hair loss specialist can use dermoscopy to measure follicle density and diameter objectively. This removes the guesswork from self-assessment.
Preparing well for that first appointment makes a real difference. A consultation preparation guide can help you arrive with the right information and questions ready.
Pro Tip: Do not wait until you can see scalp through your hair. By that point, a meaningful proportion of follicles have already miniaturised. Acting on early signs gives treatments the best chance of working.
What treatments are available for crown hair loss?
Pattern hair loss management should focus on preventing follicle damage early rather than attempting regrowth after miniaturisation is advanced. That principle shapes every treatment decision.
- Minoxidil. Applied topically or taken orally, minoxidil stimulates follicle activity and prolongs the anagen phase. It works best on follicles that are miniaturising but not yet dormant.
- Finasteride. This oral medication blocks DHT production, slowing the miniaturisation process. Both minoxidil and finasteride primarily stabilise existing hair rather than regrowing fully bald areas.
- PRP therapy. Platelet Rich Plasma therapy involves injecting concentrated growth factors from your own blood into the scalp to support follicle health. It is a non-surgical option suited to early-to-moderate thinning.
- Hair transplant surgery. Follicular Unit Extraction (FUE) is the gold-standard surgical intervention for crown restoration. Healthy follicles from the donor area are transplanted to the crown, where they grow permanently. Crown hair transplants are particularly effective when the donor supply is adequate and the pattern of loss is stable.
- Lifestyle adjustments. Addressing nutritional deficiencies, reducing scalp inflammation, and avoiding traction all support the effectiveness of medical treatments.
The NHS classifies androgenetic alopecia as a cosmetic condition, which means NHS treatment access involves long waiting times. Private clinics offer faster access to treatments including hair transplants and PRP therapy, which is why many people in the UK choose private care for active management.
Key takeaways
Crown thinning is caused primarily by androgenetic alopecia, and early intervention with medical or surgical treatment produces significantly better outcomes than waiting until loss is advanced.
| Point | Details |
|---|---|
| Primary cause | Androgenetic alopecia, driven by DHT sensitivity, accounts for the vast majority of crown thinning cases. |
| Male vs female patterns | Men develop a defined vertex bald spot; women show diffuse thinning with a widening parting and preserved hairline. |
| Early detection | Hair diameter reduction is the earliest measurable sign; monthly photography aids objective monitoring. |
| Non-genetic triggers | Telogen effluvium, thyroid disease, iron deficiency, and traction alopecia can all worsen or mimic crown thinning. |
| Treatment priority | Stabilising follicles early with minoxidil, finasteride, PRP, or FUE transplant produces better results than late intervention. |
What I have learned from seeing crown thinning cases every day
The most consistent pattern I observe is delay. People notice something is changing at the crown, attribute it to a bad haircut or the wrong shampoo, and wait another two or three years before seeking advice. By that point, the window for purely medical management has often narrowed considerably.
The second pattern is unrealistic expectation in both directions. Some people expect a tablet to fully reverse years of miniaturisation. Others assume nothing can be done and do not seek help at all. The truth sits between those two positions. Minoxidil and finasteride are genuinely effective at slowing loss, and FUE transplantation can restore natural-looking density to the crown when performed by a qualified surgeon. Neither is a cure, but both are meaningful interventions when used at the right stage.
What I find most encouraging about 2026 is the quality of early detection tools now available. Dermoscopy and follicle density mapping mean a specialist can tell you precisely how far miniaturisation has progressed, which removes the uncertainty that used to make treatment decisions so difficult. Combine that with realistic expectations and a consistent treatment plan, and the outcomes are genuinely good for most people.
The psychological impact of hair thinning is real and should not be minimised. Seeking help is not vanity. It is a reasonable response to a medical condition that affects confidence and quality of life.
— Harley
Glasgowhairtransplantclinics: personalised care for crown thinning
Crown hair thinning responds best to early, expert-led intervention. Glasgowhairtransplantclinics offers a full range of treatment pathways, from non-surgical PRP therapy to Follicular Unit Extraction (FUE) hair transplant surgery, all delivered by GMC-registered surgeons at CQC-registered clinics across the UK.
Whether you are in the early stages of noticing a thinning crown or considering surgical restoration, a free consultation is the right starting point. The team at Glasgowhairtransplantclinics will assess your follicle health, explain your options clearly, and give you a realistic picture of what treatment can achieve. You can also review transparent treatment pricing before you commit to anything. Book your free consultation at Glasgowhairtransplantclinics today.
FAQ
What is the main cause of crown hair thinning?
Androgenetic alopecia, caused by genetic sensitivity to DHT, accounts for the vast majority of crown thinning cases in both men and women. DHT shrinks hair follicles progressively, producing finer hairs until growth stops.
Can crown hair thinning be reversed?
Treatments like minoxidil and finasteride can stabilise loss and improve density in miniaturising follicles, but they do not fully reverse advanced baldness. FUE hair transplant surgery offers the most reliable restoration for areas where follicles are no longer active.
At what age does crown thinning typically start?
Follicle miniaturisation can begin in the late teens or early twenties, though visible thinning often does not appear until the thirties or forties. Early signs include finer hair strands rather than obvious bald patches.
How do I know if my crown thinning is genetic or caused by something else?
A professional assessment using dermoscopy can distinguish androgenetic alopecia from telogen effluvium, thyroid-related loss, or traction alopecia. Blood tests to rule out iron deficiency and thyroid disease are a standard part of that evaluation.
Does the NHS treat crown hair loss?
The NHS classifies androgenetic alopecia as a cosmetic condition, so NHS treatment involves long waiting times and limited options. Private clinics provide faster access to treatments including PRP therapy and hair transplant surgery.
Recommended









